

Volume 9, Issue 3 (7-2023)
Journal of Research in Applied and Basic Medical Sciences 2023, 9(3): 183-192 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
M P K R, Fatima R, Karamchedu S, Punjala M G, Patale V, K F N et al . Study of gastrointestinal neoplasms, histopathologic and immunohistochemical correlation using HER-2/NEU, CK-7 and CK-20. Journal of Research in Applied and Basic Medical Sciences 2023; 9 (3) :183-192
URL: http://ijrabms.umsu.ac.ir/article-1-255-en.html
URL: http://ijrabms.umsu.ac.ir/article-1-255-en.html
Pramod Kumar Reddy M 

 , Rasheed Fatima * , Shilpa Karamchedu , Manisha Goud Punjala , Vishali Patale , Florence N K , Suresh K
, Rasheed Fatima * , Shilpa Karamchedu , Manisha Goud Punjala , Vishali Patale , Florence N K , Suresh K
, Rasheed Fatima * , Shilpa Karamchedu , Manisha Goud Punjala , Vishali Patale , Florence N K , Suresh K
Professor, Department of Pathology, SVS Medical College and Hospital, Yenugonda, Mahabubnagar, Telangana-509001, India. , drrasheedfatima786@gmail.com
Full-Text [PDF 637 kb]
(420 Downloads)
| Abstract (HTML) (613 Views)
Table 3. showing the TNM staging
Table 4. Showing the CK20 status and histopathology
2.63% of adenocarcinomas, all mixed adeno-neuroendocrine, 60% of mucinous adenocarcinomas and 66.66% of signet ring cell carcinomas were positive for Her2neu. 18.42% of adenocarcinomas, 50% of mixed adeno-neuroendocrine, and 66.66% of signet ring cell carcinomas were positive for CK7. 21.05% of adenocarcinomas, all mucinous adenocarcinomas, and 33.33% of signet ring cell carcinomas were positive for CK20.
A total of 50 patients with gastro intestinal cancer and their samples analysed IHC to identify the significance of IHC and its correlation made between the HER-2/NEU and cytokeratins with GI neoplasms.
In our current study, majority 34% belonged to age group of 40-49 years followed by 50-59 years (26%), 60-69 years (22%), 12% belonged to the age group of 30-39 years, and 6% are > 70 years. Majority of the study population belonged to the age group of 41-60 years (47%) (14).
In the present study among the study population, sixty percent were male and 40% were female.
A study showed there was a male predominance with the male-to-female ratio of 1.67:1 (14), as out of 180 cases, 108 were males and 72 were females (15).
In the present study among the study population, adenocarcinoma was diagnosed in 76% followed by mucinous adenocarcinoma in 10%, signet cell ring cell carcinoma in 6%, and mixed adeno-neuroendocrine tumor in 4%. Sarcoma and papillary adenocarcinoma contributed to 2% each.
Whereas a study showed that most common type of cancer was diffuse type which accounted for 61%, followed by intestinal type accounting for 29%, while 10% among the cancer types were kept in others due to the unavailability of their classification in any of the given types (16). Another study conducted on gastric carcinoma showed a similar increased incidence of diffuse subtype over intestinal adenocarcinoma (17).
Histologically adenocarcinoma was main type comprising 67% followed by squamous cell carcinoma which makes up 28% of all malignancies. Other histological variants found in a study were round cell tumor in 2%, gastrointestinal stromal tumor in 2%, and adenosquamous carcinoma 1% (15).
A study showed the varied pattern with pure membranous (16%), membranous cytoplasmic (58%), and cytoplasmic (26%) staining for HER-2 immunohistochemistry (18).
Sections that showed membranous positivity (±cytoplasmic stain) were considered to be true positive for HER-2 overexpression; therefore, for intestinal and diffuse adenocarcinoma, the positivity was found to be 100% and 58% (P = 0.029) (19).
In the present study, 60% were of grade II, 32% were of grade III, and 6% were of grade I. Low-grade sarcoma was present in 2%.
In the present study, well-differentiated tumors were 6%, moderately differentiated tumors were 60%, and poorly differentiated tumors were 32%.
In the present study, 16% were positive for Her 2 neu, 20% were positive for CK7, and CK20 was positive among 28%.
Al-Maghrabi et al. study shows that the expression of CK20/CK7 is an approved diagnostic tool to determine the site of origin in metastatic carcinoma. Occasionally, the loss of expression of CK20 and conversely positive expression of CK 7 was noted in some colorectal carcinomas (CRC). In primary CRC, CK20 was positive in 62.5%, while CK7 was positive in 5.6%. In nodal metastasis, CK 20 and CK 7 showed positivity in 63.5% and 4.1%, respectively. There was no statistically significant correlation between CK20/CK7 immunohistochemical profile and clinicopathological characteristics, prognosis, and survival were identified (20).
In the present study, among the study population, 2.63% of adenocarcinomas, all of mixed adeno-neuroendocrine, 60% of mucinous adenocarcinomas, and 66.66% of signet ring cell carcinomas were positive for Her2neu.
Adenocarcinoma showed significantly higher cytoplasmic staining. Cytoplasmic staining for antibodies against HER-2/neu protein was occasionally observed Block et al. and was regarded as non-specific and excluded from the assessment of membrane staining intensity (20).
In the present study, among the study population, 18.42% of adenocarcinomas, 50% of mixed adeno-neuroendocrine, and 66.66% of signet ring cell carcinomas were positive for CK7.
In the present study, among the study population, 21.05% of adenocarcinomas, all of mucinous adenocarcinomas, and 33.33% of signet ring cell carcinomas were positive for CK20.
Deori, B. J., et al. studied 52 cases of colorectal carcinoma and Immunohistochemical staining of cytokeratin (CK) 20 was done and expression was studied and correlated with age, location of tumour, grade and tumour stage. On immunohistochemistry, CK20 expression was identified in 82.7% of colorectal adenocarcinoma and negative in 17.3% cases (22).
Kende AI et al. studied for immunohistochemical expression of CK7 and CK20 in gastrointestinal tract Lesions and shows that adenocarcinomas of the upper GI tract were +ve for both CK7 and CK20 in 78% of cases; only poorly differentiated lesions were CK7–. Well-differentiated and moderately differentiated adenocarcinomas of the large intestine/appendix were CK7–/CK20+ in the majority of cases. All five high-grade neuroendocrine carcinomas were -ve for both CK7 and CK20 (23).
In a study done by Chu P et al. (21)., the vast majority of cases of adenocarcinomas were positive for CK 7, including lung (100%), ovary (100%), uterus (100%), breast (96%), salivary gland (100%), thyroid neoplasms (100%), cholangiocarcinoma (93%), pancreas (92%), and transitional cell carcinoma (88%). In contrast, only a small percentage of cases of adenocarcinoma of colon (5%), stomach (28%), and kidney (11%) were CK 7-positive. All cases of colon carcinoma were positive for CK 20, as were most cases of Merkel cell tumor of skin (78%) and adenocarcinoma of the pancreas (62%). One-half of cases of adenocarcinoma of the stomach were CK 20-positive, as were a subset of cases of cholangiocarcinoma of the liver (43%) and transitional cell carcinoma of the bladder (29%).
In another study done by Pandey I et al. (16), only one case out of 28 cases was negative for Her2 neu staining.
Conclusion
Moderately differentiated tumors were 60%. There was no correlation between the histopathology status and receptor positivity. 16% were positive for Her 2 neu, 20% were positive for CK7, and CK20 was positive among 28%. Studies with higher sample size are required to understand the utility of HER2 expression to clarify the relationship between the HER2 protein, CK7, CK20, and clinicopathological parameters.
Acknowledgments
No Declared
Conflict of interest
No conflict of interest declaration between the authors.
Funding/support
The SVS Medical College and Hospital financially supported this study.
Full-Text: (253 Views)
Introduction
Globally stomach cancer is the fifth-leading cause of cancer and the third leading cause of death from cancer, making up to 7% of cases and 9% of deaths (1). In India, gastric cancer is ranked the 5th and 7th most common cancer in males and females, respectively, and is the second leading cause of death from cancer in both men and women (2). Lifetime risk of development of gastric cancer is 1.5% (3). An association between clinicopathological features and molecular markers like HER-2 for gastric adenocarcinoma could give a clue toward the relationship between them and hence provide us an extra tool to combat the high mortality due to these carcinomas. Targeted therapy toward HER-2/neu can be justified only when sufficient data regarding the role of these molecules in GAC is available (4, 5).
The HER-2 protein (p185, HER-2/neu, ErbB-2) is a 185-kDa transmembrane tyrosine kinase (TK) receptor and a member of the epidermal growth factor receptors (EGFRs) family. In addition to breast carcinoma, recent studies have also reported an overexpression of HER-2/neu in a subset of 6%–30% of patients with gastric adenocarcinoma.
HER-2 positive gastric carcinomas are usually of the gland-forming intestinal type, and may show complete, basolateral or lateral staining in addition to complete membrane staining (6). HER-2 expression has become an important biomarker for identifying patients who could respond to HER-2 targeting therapy using the fully humanized monoclonal antibody trastuzumab.
Although membranous overexpression of HER-2 is low in colorectal cancer and only 5% of all patients being positive, a significant proportion of the patients (30%) shows cytoplasmic HER-2 overexpression. Half et al. (7) analyzed the localization of cytoplasmic HER-2 in colorectal cancer. In the study of Jindal et al., 44.44% cases of intestinal type adenocarcinoma of stomach showed only membrane staining, whereas 55.56% cases showed both membranous and cytoplasmic staining. In diffuse adenocarcinoma group, membranous and membranous+cytoplasmic staining were present in 14.63% and 41.43%, respectively. 31.71% of the cases had only cytoplasmic staining without any evidence of membranous positivity. Also 12.20% were negative for HER-2 expression (8).
CK20 is expressed alone in the majority of intestinal adenocarcinoma and in Merkel cell carcinomas, whereas CK7 is present without CK20 in most breast, lung and ovarian adenocarcinoma, and with CK20 in urothelial, pancreatic, and gastric carcinomas. The CK7-/CK20+ expression pattern is known to be highly characteristic of colorectal carcinomas, however, not all colorectal carcinomas show the CK7-/CK20+ expression pattern. Occasionally colorectal carcinomas may show significant CK7 expression and conversely, expression of CK20 may be seen in a variety of non-colorectal adenocarcinomas such as urothelial, gastric, and pancreatobiliary tract carcinomas (9-13).
The present study was taken up to study the significance of IHC and its correlation using HER-2/NEU and cytokeratins in histopathologic study of GI neoplasms.
Materials & Methods
The study was conducted in the Department of Pathology, SVS Medical College and Hospital. It is the tertiary care center situated in Mahaboobnagar. Ethical clearance was obtained from the Institutional Ethical Committee, SVS College and Hospital, Mahaboobnagar.
Type of Study: SEP 2018-2020 (retrospective), SEP 2020-2022 (prospective).
Sampling Method: Convenient sampling.
Study Population: Total of 50 Patients presenting with gastro-intestinal cancer and their samples sent for IHC to Department of Pathology, SVS Hospital.
Methodology:
Patients presenting with gastrointestinal cancer and their samples sent for IHC to Department of Pathology, SVS Hospital, satisfying the inclusion criteria were enrolled into the study and admitted after getting informed consent from them.
Inclusion Criteria:
• Patients with all relevant clinical history and investigations presenting with malignant gastro-intestinal tumors.
• Patients with the above-mentioned criteria who are willing to give informed consent.
Exclusion criteria:
• Patients with benign lesions
• Malignant tumors of Esophagus, Pancreas, Liver, and Gallbladder
• Patients who are not willing to participate in the study.
Procedure:
The data was entered in a pre-tested semi-structured questionnaire. All the patients who met the inclusion criteria were taken up for the study.
Staining and IHC:
Two micro sections of 4 to 5-micron thickness were prepared from the corresponding paraffin blocks, one on albumin coated slide for H&E staining and the other on Poly-L-lysine coated slide for immune-histochemical staining. Invasive breast carcinoma histological typing and histological grading (I, II, and III) was done according to Elston33, using the scale assigned to three features: tubular formation (1 to 3), nuclear atypia (1 to 3), and mitoses (1 to 3).
Statistics: The data was analysed using the Statistical Package for Social Science Software (SPSS with Windows version 20.0, IL, USA). Results on continuous measurements were presented on Mean±SD (Min-Max) and results on categorical measurements were presented in Number (%). Significance was assessed at 5% level of significance. Student’s t‑test used to compare continuous variables between the two groups. Chi‑square (χ2) test and Fisher’s exact test were used to compare categorical parameters among two or more groups. Sensitivity, Specificity, Positive Predictive Value, Negative predictive value, Diagnostic accuracy were calculated using the Histopathological findings as gold standard. The P < 0.05 was considered statistically significant.
Results
Among the study population, 34% were of the age group of 40-49 years, followed by 26% in 50-59 years, 22% in 60-69 years, 12% of 30-39 years, and 6% of > 70 years age group, respectively. Sixty percent were male and 40% were female.
Globally stomach cancer is the fifth-leading cause of cancer and the third leading cause of death from cancer, making up to 7% of cases and 9% of deaths (1). In India, gastric cancer is ranked the 5th and 7th most common cancer in males and females, respectively, and is the second leading cause of death from cancer in both men and women (2). Lifetime risk of development of gastric cancer is 1.5% (3). An association between clinicopathological features and molecular markers like HER-2 for gastric adenocarcinoma could give a clue toward the relationship between them and hence provide us an extra tool to combat the high mortality due to these carcinomas. Targeted therapy toward HER-2/neu can be justified only when sufficient data regarding the role of these molecules in GAC is available (4, 5).
The HER-2 protein (p185, HER-2/neu, ErbB-2) is a 185-kDa transmembrane tyrosine kinase (TK) receptor and a member of the epidermal growth factor receptors (EGFRs) family. In addition to breast carcinoma, recent studies have also reported an overexpression of HER-2/neu in a subset of 6%–30% of patients with gastric adenocarcinoma.
HER-2 positive gastric carcinomas are usually of the gland-forming intestinal type, and may show complete, basolateral or lateral staining in addition to complete membrane staining (6). HER-2 expression has become an important biomarker for identifying patients who could respond to HER-2 targeting therapy using the fully humanized monoclonal antibody trastuzumab.
Although membranous overexpression of HER-2 is low in colorectal cancer and only 5% of all patients being positive, a significant proportion of the patients (30%) shows cytoplasmic HER-2 overexpression. Half et al. (7) analyzed the localization of cytoplasmic HER-2 in colorectal cancer. In the study of Jindal et al., 44.44% cases of intestinal type adenocarcinoma of stomach showed only membrane staining, whereas 55.56% cases showed both membranous and cytoplasmic staining. In diffuse adenocarcinoma group, membranous and membranous+cytoplasmic staining were present in 14.63% and 41.43%, respectively. 31.71% of the cases had only cytoplasmic staining without any evidence of membranous positivity. Also 12.20% were negative for HER-2 expression (8).
CK20 is expressed alone in the majority of intestinal adenocarcinoma and in Merkel cell carcinomas, whereas CK7 is present without CK20 in most breast, lung and ovarian adenocarcinoma, and with CK20 in urothelial, pancreatic, and gastric carcinomas. The CK7-/CK20+ expression pattern is known to be highly characteristic of colorectal carcinomas, however, not all colorectal carcinomas show the CK7-/CK20+ expression pattern. Occasionally colorectal carcinomas may show significant CK7 expression and conversely, expression of CK20 may be seen in a variety of non-colorectal adenocarcinomas such as urothelial, gastric, and pancreatobiliary tract carcinomas (9-13).
The present study was taken up to study the significance of IHC and its correlation using HER-2/NEU and cytokeratins in histopathologic study of GI neoplasms.
Materials & Methods
The study was conducted in the Department of Pathology, SVS Medical College and Hospital. It is the tertiary care center situated in Mahaboobnagar. Ethical clearance was obtained from the Institutional Ethical Committee, SVS College and Hospital, Mahaboobnagar.
Type of Study: SEP 2018-2020 (retrospective), SEP 2020-2022 (prospective).
Sampling Method: Convenient sampling.
Study Population: Total of 50 Patients presenting with gastro-intestinal cancer and their samples sent for IHC to Department of Pathology, SVS Hospital.
Methodology:
Patients presenting with gastrointestinal cancer and their samples sent for IHC to Department of Pathology, SVS Hospital, satisfying the inclusion criteria were enrolled into the study and admitted after getting informed consent from them.
Inclusion Criteria:
• Patients with all relevant clinical history and investigations presenting with malignant gastro-intestinal tumors.
• Patients with the above-mentioned criteria who are willing to give informed consent.
Exclusion criteria:
• Patients with benign lesions
• Malignant tumors of Esophagus, Pancreas, Liver, and Gallbladder
• Patients who are not willing to participate in the study.
Procedure:
The data was entered in a pre-tested semi-structured questionnaire. All the patients who met the inclusion criteria were taken up for the study.
Staining and IHC:
Two micro sections of 4 to 5-micron thickness were prepared from the corresponding paraffin blocks, one on albumin coated slide for H&E staining and the other on Poly-L-lysine coated slide for immune-histochemical staining. Invasive breast carcinoma histological typing and histological grading (I, II, and III) was done according to Elston33, using the scale assigned to three features: tubular formation (1 to 3), nuclear atypia (1 to 3), and mitoses (1 to 3).
Statistics: The data was analysed using the Statistical Package for Social Science Software (SPSS with Windows version 20.0, IL, USA). Results on continuous measurements were presented on Mean±SD (Min-Max) and results on categorical measurements were presented in Number (%). Significance was assessed at 5% level of significance. Student’s t‑test used to compare continuous variables between the two groups. Chi‑square (χ2) test and Fisher’s exact test were used to compare categorical parameters among two or more groups. Sensitivity, Specificity, Positive Predictive Value, Negative predictive value, Diagnostic accuracy were calculated using the Histopathological findings as gold standard. The P < 0.05 was considered statistically significant.
Results
Among the study population, 34% were of the age group of 40-49 years, followed by 26% in 50-59 years, 22% in 60-69 years, 12% of 30-39 years, and 6% of > 70 years age group, respectively. Sixty percent were male and 40% were female.
Table 1. site of the tumor and their frequency
Table 2. Size of the tumor and their frequency
| site of the tumor | Frequency | Percentage |
| Antrum of Stomach | 1 | 2 |
| Ascending Colon | 5 | 10 |
| Descending Colon | 1 | 2 |
| Ileocecal junction | 2 | 4 |
| Ileum | 1 | 2 |
| Jejunum | 3 | 6 |
| Rectosigmoid | 8 | 16 |
| Rectum | 9 | 18 |
| size of the tumor | Frequency | Percentage |
| 12cm | 1 | 2 |
| 2cm | 1 | 2 |
| 3cm | 4 | 8 |
| 4cm | 8 | 16 |
| 5cm | 19 | 38 |
| 6cm | 10 | 20 |
| 7cm | 5 | 10 |
| 8cm | 1 | 2 |
| 9cm | 1 | 2 |
| Grand Total | 50 | 100 |
Among the study population, adenocarcinoma was diagnosed in 76%, followed by mucinous adenocarcinoma in 10%, signet cell ring cell carcinoma in 6%, and mixed adeno-neuroendocrine tumor in 4%. Sarcoma and papillary adenocarcinoma contributed to 2% each. In total, 60% were of grade II, 32% were of grade III, and 6% were of grade I. Low-grade sarcoma was present in 2%.
Table 3. showing the TNM staging
| TNM staging | Frequency | Percentage |
| - | 1 | 2 |
| PT1aN0M0 | 1 | 2 |
| PT2N0M0 | 11 | 22 |
| PT2N0M1 | 1 | 2 |
| PT2NXM0 | 1 | 2 |
| PT3N0M0 | 14 | 28 |
| PT3N1bM0 | 3 | 6 |
| PT3N1cM0 | 1 | 2 |
| PT3N1M0 | 2 | 4 |
| PT3N2bM0 | 1 | 2 |
| PT3N2M0 | 1 | 2 |
| PT3N3bM0 | 3 | 6 |
| PT3NXM0 | 2 | 4 |
| PT3NXMX | 1 | 2 |
| PT4aNXM0 | 2 | 4 |
| PT4bN0M0 | 1 | 2 |
| PT4N0M0 | 1 | 2 |
| PT4N1aM0 | 2 | 4 |
| PT4NXM0 | 1 | 2 |
| Grand Total | 50 | 100 |
In this study, well-differentiated tumors were 6%, moderately differentiated tumors were 60%, and poorly differentiated tumors were 32%. Totally 16% were positive for Her 2 neu, 20% were positive for CK7, and CK20 was positive among 28%.
Table 4. Showing the CK20 status and histopathology
| Histopathology | CK20 Positive | CK7 Positive | HER2NEU Positive | Grand Total |
| Moderately differentiated | 8 | 4 | 3 | 30 |
| Poorly differentiated | 4 | 6 | 4 | 16 |
| Well differentiated | 2 | 0 | 1 | 3 |
| Grand Total | 14 | 10 | 8 | 49 |
2.63% of adenocarcinomas, all mixed adeno-neuroendocrine, 60% of mucinous adenocarcinomas and 66.66% of signet ring cell carcinomas were positive for Her2neu. 18.42% of adenocarcinomas, 50% of mixed adeno-neuroendocrine, and 66.66% of signet ring cell carcinomas were positive for CK7. 21.05% of adenocarcinomas, all mucinous adenocarcinomas, and 33.33% of signet ring cell carcinomas were positive for CK20.
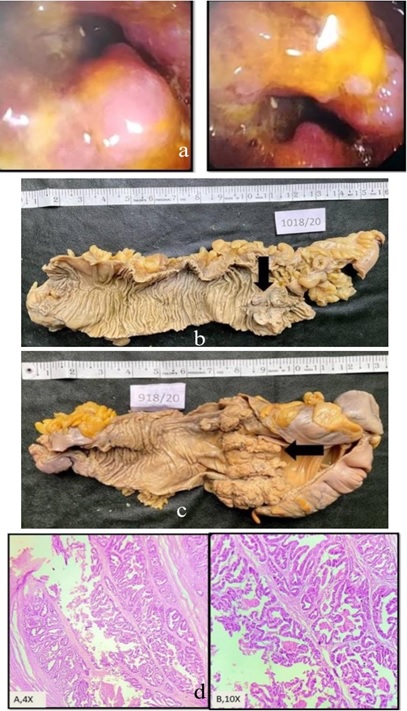
Fig. 1. Well differentiated adenocarcinoma. a. Colonoscopy picture showing ulceroproliferative growth. b. Gross picture of Right Hemicolectomy showing ulceroproliferative. c. Gross picture of Right Hemicolectomy showing large polypoidal growth in the ascending colon. d. H&E 10x & 40x, microscopically, a well-differentiated adenocarcinoma of colon showing well-formed glandular configuration with uniform basally oriented nuclei.
Table 5. showing the HER 2 NEU status and diagnosis

Fig. 2. a. Moderately differentiated Adenocarcinoma. H&E 10X, Microscopically showing multiple glands which are irregular and crowded. b. H&E 40X showing loss of nuclear polarity. c. Poorly differentiated Adenocarcinoma. H&E 10X- Microscopically tumor consists of sheets of round to oval cells without gland formation. d. H&E 40X – Nuclear pleomorphism and prominent nucleoli. e&f. Mucinous Adenocarcinoma. H&E Sections, showing mucinous adenocarcinoma with large mucinous pools with tumor cells floating in the extracellular mucin.
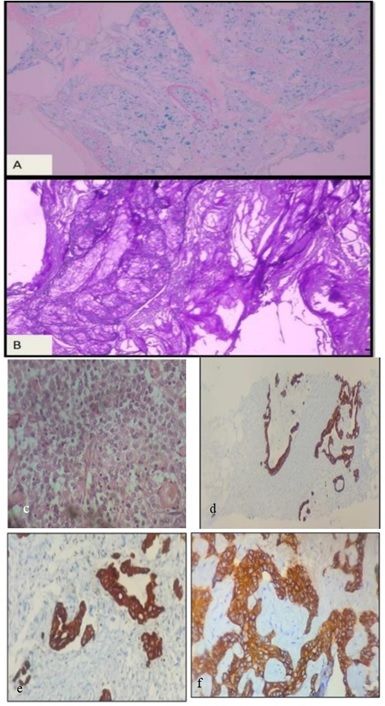
Fig. 3. a&b. Special stains for mucinous adenocarcinoma. c. H&E sections, A showing sheets of large cells resembling neuroendocrine features. D.CK20 positive (10X). e. CK7 positive (40X). f. Her2/neu positive (40X).
DiscussionTable 5. showing the HER 2 NEU status and diagnosis
| Diganosis | Her 2 neu Positive | CK7 Positive | CK20 Positive | Total |
| Adenocarcinoma | 1(2.63%) | 7(18.42%) | 8 (21.05%) | 38(100%) |
| Low-grade Sarcoma | 0 | 0 | 0 | 1(100%) |
| Mixed Adenoneuroendocrine | 2(100%) | 1(50%) | 0 | 2(100%) |
| Mucinous Adenocarcinoma | 3(60%) | 0 | 5(100%) | 5(100%) |
| Papillary Adenocarcinoma | 0 | 0 | 0 | 1(100%) |
| Signet ring cell carcinoma | 2(66.66%) | 2(66.66%) | 1(33.33%) | 3(100%) |
| Grand Total | 8(16%) | 10(20%) | 14(28%) | 50(100%) |
Fig. 2. a. Moderately differentiated Adenocarcinoma. H&E 10X, Microscopically showing multiple glands which are irregular and crowded. b. H&E 40X showing loss of nuclear polarity. c. Poorly differentiated Adenocarcinoma. H&E 10X- Microscopically tumor consists of sheets of round to oval cells without gland formation. d. H&E 40X – Nuclear pleomorphism and prominent nucleoli. e&f. Mucinous Adenocarcinoma. H&E Sections, showing mucinous adenocarcinoma with large mucinous pools with tumor cells floating in the extracellular mucin.
Fig. 3. a&b. Special stains for mucinous adenocarcinoma. c. H&E sections, A showing sheets of large cells resembling neuroendocrine features. D.CK20 positive (10X). e. CK7 positive (40X). f. Her2/neu positive (40X).
A total of 50 patients with gastro intestinal cancer and their samples analysed IHC to identify the significance of IHC and its correlation made between the HER-2/NEU and cytokeratins with GI neoplasms.
In our current study, majority 34% belonged to age group of 40-49 years followed by 50-59 years (26%), 60-69 years (22%), 12% belonged to the age group of 30-39 years, and 6% are > 70 years. Majority of the study population belonged to the age group of 41-60 years (47%) (14).
In the present study among the study population, sixty percent were male and 40% were female.
A study showed there was a male predominance with the male-to-female ratio of 1.67:1 (14), as out of 180 cases, 108 were males and 72 were females (15).
In the present study among the study population, adenocarcinoma was diagnosed in 76% followed by mucinous adenocarcinoma in 10%, signet cell ring cell carcinoma in 6%, and mixed adeno-neuroendocrine tumor in 4%. Sarcoma and papillary adenocarcinoma contributed to 2% each.
Whereas a study showed that most common type of cancer was diffuse type which accounted for 61%, followed by intestinal type accounting for 29%, while 10% among the cancer types were kept in others due to the unavailability of their classification in any of the given types (16). Another study conducted on gastric carcinoma showed a similar increased incidence of diffuse subtype over intestinal adenocarcinoma (17).
Histologically adenocarcinoma was main type comprising 67% followed by squamous cell carcinoma which makes up 28% of all malignancies. Other histological variants found in a study were round cell tumor in 2%, gastrointestinal stromal tumor in 2%, and adenosquamous carcinoma 1% (15).
A study showed the varied pattern with pure membranous (16%), membranous cytoplasmic (58%), and cytoplasmic (26%) staining for HER-2 immunohistochemistry (18).
Sections that showed membranous positivity (±cytoplasmic stain) were considered to be true positive for HER-2 overexpression; therefore, for intestinal and diffuse adenocarcinoma, the positivity was found to be 100% and 58% (P = 0.029) (19).
In the present study, 60% were of grade II, 32% were of grade III, and 6% were of grade I. Low-grade sarcoma was present in 2%.
In the present study, well-differentiated tumors were 6%, moderately differentiated tumors were 60%, and poorly differentiated tumors were 32%.
In the present study, 16% were positive for Her 2 neu, 20% were positive for CK7, and CK20 was positive among 28%.
Al-Maghrabi et al. study shows that the expression of CK20/CK7 is an approved diagnostic tool to determine the site of origin in metastatic carcinoma. Occasionally, the loss of expression of CK20 and conversely positive expression of CK 7 was noted in some colorectal carcinomas (CRC). In primary CRC, CK20 was positive in 62.5%, while CK7 was positive in 5.6%. In nodal metastasis, CK 20 and CK 7 showed positivity in 63.5% and 4.1%, respectively. There was no statistically significant correlation between CK20/CK7 immunohistochemical profile and clinicopathological characteristics, prognosis, and survival were identified (20).
In the present study, among the study population, 2.63% of adenocarcinomas, all of mixed adeno-neuroendocrine, 60% of mucinous adenocarcinomas, and 66.66% of signet ring cell carcinomas were positive for Her2neu.
Adenocarcinoma showed significantly higher cytoplasmic staining. Cytoplasmic staining for antibodies against HER-2/neu protein was occasionally observed Block et al. and was regarded as non-specific and excluded from the assessment of membrane staining intensity (20).
In the present study, among the study population, 18.42% of adenocarcinomas, 50% of mixed adeno-neuroendocrine, and 66.66% of signet ring cell carcinomas were positive for CK7.
In the present study, among the study population, 21.05% of adenocarcinomas, all of mucinous adenocarcinomas, and 33.33% of signet ring cell carcinomas were positive for CK20.
Deori, B. J., et al. studied 52 cases of colorectal carcinoma and Immunohistochemical staining of cytokeratin (CK) 20 was done and expression was studied and correlated with age, location of tumour, grade and tumour stage. On immunohistochemistry, CK20 expression was identified in 82.7% of colorectal adenocarcinoma and negative in 17.3% cases (22).
Kende AI et al. studied for immunohistochemical expression of CK7 and CK20 in gastrointestinal tract Lesions and shows that adenocarcinomas of the upper GI tract were +ve for both CK7 and CK20 in 78% of cases; only poorly differentiated lesions were CK7–. Well-differentiated and moderately differentiated adenocarcinomas of the large intestine/appendix were CK7–/CK20+ in the majority of cases. All five high-grade neuroendocrine carcinomas were -ve for both CK7 and CK20 (23).
In a study done by Chu P et al. (21)., the vast majority of cases of adenocarcinomas were positive for CK 7, including lung (100%), ovary (100%), uterus (100%), breast (96%), salivary gland (100%), thyroid neoplasms (100%), cholangiocarcinoma (93%), pancreas (92%), and transitional cell carcinoma (88%). In contrast, only a small percentage of cases of adenocarcinoma of colon (5%), stomach (28%), and kidney (11%) were CK 7-positive. All cases of colon carcinoma were positive for CK 20, as were most cases of Merkel cell tumor of skin (78%) and adenocarcinoma of the pancreas (62%). One-half of cases of adenocarcinoma of the stomach were CK 20-positive, as were a subset of cases of cholangiocarcinoma of the liver (43%) and transitional cell carcinoma of the bladder (29%).
In another study done by Pandey I et al. (16), only one case out of 28 cases was negative for Her2 neu staining.
Conclusion
Moderately differentiated tumors were 60%. There was no correlation between the histopathology status and receptor positivity. 16% were positive for Her 2 neu, 20% were positive for CK7, and CK20 was positive among 28%. Studies with higher sample size are required to understand the utility of HER2 expression to clarify the relationship between the HER2 protein, CK7, CK20, and clinicopathological parameters.
Acknowledgments
No Declared
Conflict of interest
No conflict of interest declaration between the authors.
Funding/support
The SVS Medical College and Hospital financially supported this study.
Type of Study: orginal article |
Subject:
Other
References
1. Stewart BW, Wild CP, editors. World Cancer Report 2014. Lyon, France: International Agency for Research on Cancer; 2014 [URL]
2. Dikshit R, Gupta PC, Ramasundarahettige C, Gajalakshmi V, Aleksandrowicz L, Badwe R, et al. Cancer mortality in India: A nationally representative survey. Lancet 2012;379:1807-16.
https://doi.org/10.1016/S0140-6736(12)60358-4 [DOI:10.1016/s0140-6736(12)60358-4] [PMID]
3. Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin DM, Piñeros M, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer 2019;144:1941-53. [DOI:10.1002/ijc.31937] [PMID]
4. Wang HB, Liao XF, Zhang J. Clinicopathological factors associated with HER2- positive gastric cancer: A meta-analysis. Medicine (Baltimore) 2017;96:e8437.
https://doi.org/10.1097/MD.0000000000008437 [DOI:10.1097/md.0000000000008437] [PMID] []
5. Hofmann M, Stoss O, Shi D, Büttner R, van de Vijver M, Kim W. Assessment of a HER2 scoring system for gastric cancer: Results from a validation study. Histopathology 2008;52:797-805. [DOI:10.1111/j.1365-2559.2008.03028.x] [PMID]
6. Mabula JB, McHembe MD, Koy M, Chalya PL, Massaga F, Rambau PF, et al. Gastric cancer at a university teaching hospital in northwestern Tanzania: A retrospective review of 232 cases. World J Surg Oncol 2012;10:257. [DOI:10.1186/1477-7819-10-257] [PMID] []
7. Half E, Broaddus R, Danenberg KD, Danenberg PV, Ayers GD, Sinicrope FA. HER-2 receptor expression, localization, and activation in colorectal cancer cell lines and human tumors. Int J Cancer 2004;108:540-8. [DOI:10.1002/ijc.11599] [PMID]
8. Jindal Y, Varma K, Misra V, Kumar R, Singh A, Misra SP, et al. Cytoplasmic expression of HER2 in gastric adenocarcinoma: An unusual finding. Indian J Med Res Pharm Sci 2016;3. [Google Scholar]
9. Hernandez BY, Frierson HF, Moskaluk CA, Li YJ, Clegg L, Cote TR, McCusker ME, Hankey BF, Edwards BK, Goodman MT: CK20 and CK7 protein expression in colorectal carcinoma: demonstration of the utility of a population-based tissue microarray. Hum Pathol 2005;36:275-81. [DOI:10.1016/j.humpath.2005.01.013] [PMID]
10. Zhang PJ, Shah M, Spiegel GW, Brooks JJ: Cytokeratin 7 immunoreactivity in rectal adenocarcinomas. Appl Immunohistochem Mol Morphol 2003;11:306-10. [DOI:10.1097/00129039-200312000-00005] [PMID]
11. Park SY, Kim HS, Hong EK, Kim WH: Expression of cytokeratins 7 and 20 in primary carcinomas of the stomach and colorectum andt heirvalue in the differential diagnosis of metastatic carcinomas to the ovary. Hum Pathol 2002;33:1078-85. [DOI:10.1053/hupa.2002.129422] [PMID]
12. Rullier A, Le Bail B, Fawaz R, Blanc JF, Saric J, Bioulac-Sage P: Cytokeratin 7 and 20 expression in cholangiocarcinomas varies along the biliary tract but stil differs from that in colorectal carcinomas metastasis. Am J Surg Pathol 2000;24:870-6. [DOI:10.1097/00000478-200006000-00014] [PMID]
13. Drummond F, Putt W, Fox M, Edwards YH: Cloning and chromosome assignment of the human CDX2 gene. Ann Hum Genet 1997;393-400.
https://doi.org/10.1017/S0003480097006465 [DOI:10.1017/s0003480097006465] [PMID]
14. Parmar A, Kokani M. J, Patel M. A study of neoplast ic study of gastrointestinal tumors. Trop J Path Micro 2018;4(1):27-33. [DOI:10.17511/jopm.2018.i01.05]
15. Mahajan, Mahajan NA, Kale SS, Bhale CP. Histopathology of Gastrointestinal Tract Malignancies - A Two Year Retrospective Study. Annals of Pathology and Laboratory Medicine, Vol. 4, Issue 4, July-August, 2017
https://doi.org/10.21276/APALM.1246 [DOI:10.21276/apalm.1246]
16. Pandey I, Misra V, Pandey AT, Verma A. Expression of HER2/neu in gastric adenocarcinoma and its correlation with serum HER2/neu level and E-cadherin expression. Indian J Pathol Microbiol 2022;65:35-41. [Google Scholar]
17. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: The results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer 2011;11:69-77. [DOI:10.5230/jgc.2011.11.2.69] [PMID] []
18. Gill MK, Jain K, Manjari M, Kaur T. Expression of Her-2/neu in colon carcinoma and its correlation with the histological grades and the lymph nodes status. J Clin Diagn Res 2011;5:1564-8. [Google Scholar]
19. Iqbal N, Iqbal N. Human Epidermal Growth Factor Receptor 2 (HER2) in cancers: Overexpression and therapeutic implications. Mol Biol Int 2014;2014:852748 [DOI:10.1155/2014/852748] [PMID] []
20. Blok EJ, Kuppen PJ, van Leeuwen JE, Sier CF. Cytoplasmic overexpression of HER2: A key factor in colorectal cancer. Clin Med Insights Oncol 2013;7:41-51
https://doi.org/10.4137/CMO.S10811 [DOI:10.4137/cmo.s10811] [PMID] []
21. Chu P, Wu E, Weiss, L. Cytokeratin 7 and Cytokeratin 20 Expression in Epithelial Neoplasms: A Survey of 435 Cases. Mod Pathol 2000.13, 962-972. [DOI:10.1038/modpathol.3880175] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Address: Urmia University of Medical Sciences, Jahad Ave., Urmia, I.R. Iran. Post code: 57147-83734. P.O. Box. 1138
Email: ijrabms gmail.com
gmail.com
rabmsumsu.ac.ir
Tel / Fax: +984431937332/+984432240642
