



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ijrabms.umsu.ac.ir/article-1-342-en.html


 , Hafiz Khush Naseeb Ahmad , Hameeda Naheed , Hina Manzoor , Jamila Shuja , Awais-ur- Rehman , Imran Arif , Muhammad Sadiq , Shagufta Kanwal , Shehla Iftikhar
, Hafiz Khush Naseeb Ahmad , Hameeda Naheed , Hina Manzoor , Jamila Shuja , Awais-ur- Rehman , Imran Arif , Muhammad Sadiq , Shagufta Kanwal , Shehla Iftikhar
Introduction
The use of radioactive sources spans various fields, including agriculture, industry, research, medicine, and education, providing numerous benefits. Advances in healthcare and an aging population have increased the use of radiation and radionuclides for diagnostic and therapeutic purposes (1). While the general public is typically exposed to low-level background radiation from natural sources, medical equipment such as nuclear medicines and X-rays—both industrial and diagnostic—constitute the primary sources of man-made radiation exposure, accounting for approximately 4% and 11% of exposure respectively (2).
Most exposure to low radiation doses occurs through medical and occupational contexts involving ionizing radiation. Research indicates that cancer risk correlates directly with the absorbed radiation dose, underscoring the importance of developing models to understand the carcinogenic effects of low-level exposure (3). The International Commission on Radiological Protection (ICRP) aims to provide a comprehensive system and practical guidelines for radiation protection, addressing exposure controls across medical, occupational, and environmental settings to prevent radiological incidents without hindering beneficial practices (4).
Occupational exposure refers to the exposure of workers to ionizing radiation in their workplace, excluding exposures not covered by standards or those exempt from regulation (5). For workers exposed to medical radiation sources, adherence to the guidelines in the International Basic Safety Standards for Protection against Ionizing Radiation and the Safety of Radiation Sources is crucial. Government agencies and organizations must consider dose calculations for radiation workers when assessing radiation hazards and implementing protective measures (6).
The principle of Time-Distance-Shielding (TDS) is central to radiation safety, aiming to protect workers and the public from man-made radiation sources. If reducing exposure time is not feasible, maintaining a safe distance from the source can minimize exposure. When neither time reduction nor distancing is possible, proper shielding between the source and the subject is essential. Various devices and materials, such as lead glass, concrete walls, and lead bricks, are used to shield against unnecessary radiation (7).
In the southwest region of Pakistan, Quetta—the capital of Baluchistan—hosts the Centre for Nuclear Medicine and Radiotherapy (CENAR), the sole cancer management center in the province. CENAR is dedicated to providing exceptional cancer care and ensuring patient satisfaction. It employs both sealed and unsealed radiation sources, as well as man-made radiation-generating machines, for therapeutic and diagnostic purposes. In the nuclear medicine department, Tc 99m and I-131 are used for routine diagnostics and treating thyroid conditions, while X-ray and mammography units are used in the radiology department. The radiotherapy department utilizes Linear Accelerators (LINAC) and Co-60 for cancer treatments.
Monitoring and measuring radiation is crucial for ensuring appropriate protection. One of the primary tools for personal dosimetry is the film badge, which monitors employees in radiation-prone areas. The film badge, containing a photographic film within a plastic holder, differentiates between beta, X-ray, gamma, and neutron radiations, and assesses individual doses through open windows and various filters (8). Developing the film from these badges reveals the optical density, total dose, and contributions from each type of radiation (9).
Adhering to standards set by the International Atomic Energy Agency (IAEA) and the International Commission on Radiological Protection (ICRP), the Pakistan Nuclear Regulatory Authority (PNRA) has established a permissible occupational dose level of 20 mSv for radiation workers in Pakistan (10). This study compares the radiation doses received by CENAR employees to the limits established by national and international regulatory agencies.
Materials & Methods
This observational research was conducted at CENAR in Quetta to monitor occupational radiation doses. Each employee handling radioactive material at CENAR is given a film badge with a unique identifying number. Each month, PINSTECH (Pakistan Institute of Nuclear Science and Technology) in Islamabad delivers the film badges. The measuring of an employee's occupational radiation exposure is advised for radiation workers using a film badge as part of their personnel monitoring system (9).
In this study, the radiation dose received in the year 2019 (January-December 2019) and the total dose expected in the last five years (January 2019- December 2023) by 35 radiation workers of CENAR, Quetta were assessed. To assess the workers' history of radiation exposure, the readings from the film badges that PINSTECH gave have been retained as records. Data analysis involved department-specific evaluation of radiation doses, comparison with established safety limits, and assessment of trends over the five years. The study additionally examined compliance with annual radiation exposure limits. While the descriptive nature of the study design provides valuable insights, it is limited in establishing causal relationships and generalizability of findings beyond the observed data. The relatively small sample size of 35 participants necessitates further investigation with a larger cohort to enhance the generalizability of the results.
Results
For staff exposure limits to remain below the levels recommended by the International Commission on Radiological Protection (ICRP) in 1991 (as amended), personnel radiation monitoring is necessary (11). The total number of radiation workers working in CENAR, Quetta mentioned in Figure-1.
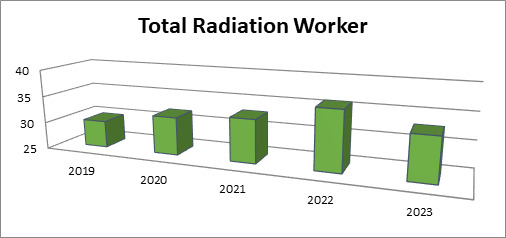
Fig. 1. Total Number of radiation workers from 2019 to 2023
Department wise Distribution among the years 2019 to 2023 is shown in Figure-2.
.jpg)
Fig. 2. Department Wise Distribution from 2019 to 2023
Departmental wise average dose distribution is shown as in Table-1.
Table 1. Departmental wise average dose distribution
|
Department |
Year |
Total Workers |
Total Dose |
Average Dose of Worker (mSv) |
percent of Permissible Limit i.e., (20 mSv) |
|
Radiotherapy |
2019 |
14 |
16.8 |
1.2 |
6 |
|
2020 |
15 |
15.45 |
1.03 |
5.15 |
|
|
2021 |
14 |
13.02 |
0.93 |
4.65 |
|
|
2022 |
14 |
14.14 |
1.01 |
5.05 |
|
|
2023 |
13 |
15.6 |
1.2 |
6 |
|
|
Nuclear Medicine |
2019 |
5 |
6.2 |
1.24 |
6.2 |
|
2020 |
7 |
6.93 |
0.99 |
4.95 |
|
|
2021 |
8 |
9 |
1.125 |
5.625 |
|
|
2022 |
10 |
10 |
1 |
5 |
|
|
2023 |
8 |
9.6 |
1.2 |
6 |
|
|
Radiology |
2019 |
2 |
2.4 |
1.2 |
6 |
|
2020 |
2 |
2.4 |
1.2 |
6 |
|
|
2021 |
3 |
2.7 |
0.9 |
4.5 |
|
|
2022 |
4 |
4.3 |
1.075 |
5.375 |
|
|
2023 |
4 |
4.8 |
1.2 |
6 |
|
|
Medical Physics |
2019 |
3 |
3.6 |
1.2 |
6 |
|
2020 |
4 |
4.12 |
1.03 |
5.15 |
|
|
2021 |
4 |
4.6 |
1.15 |
5.75 |
|
|
2022 |
5 |
5.8 |
1.16 |
5.8 |
|
|
2023 |
5 |
6 |
1.2 |
6 |
|
|
Others |
2019 |
5 |
6 |
1.2 |
6 |
|
2020 |
5 |
6 |
1.2 |
6 |
|
|
2021 |
4 |
3.6 |
0.9 |
4.5 |
|
|
2022 |
4 |
4.64 |
1.16 |
5.8 |
|
|
2023 |
4 |
4.8 |
1.2 |
6 |
Discussion
The majority of radiation workers of CENAR received the annual doses less than 6% of the annual dose as shown in Table-1. The average occupational data in medical physics, radiotherapy, nuclear medicine and radiology in CENAR, Quetta between 2019 and 2023 were reported as shown as a figure in the Fugure-1 and Fugure-2. According to the Fugure-1 and Fugure-2, the data ranged from 1.03 mSv to 1.2 mSv, 0.93 mSv to 1.2 mSv, 0.99 mSv to 1.2 mSv and 0.90 mSv to 1.2 mSv respectively.
The average occupational exposure data of workers in nuclear medicine, radiotherapy, and diagnostic radiology in Pakistan between 2003 and 2007 was reported by Jabeen A et al. ranged from 1.39 mSv to 1.80 mSv, 1.05 mSv to 1.45 mSv, and 1.22 mSv to 1.71 mSv, respectively (12).
The annual doses of radiation workers in the nuclear medicine, radiotherapy, and diagnostic radiology divisions were reported by Weizhang W et al. These doses fell within the ranges of 1.2-1.6, 1.0-1.5, and 1.5-2.2 mSv, respectively (13).
According to research by Korir GK et al., 81% of radiation workers received doses in a year ranging from 1 mSv to 5 mSv, while 17% of workers had yearly doses of less than 1 mSv (14).
According to Careiro JV and Avelar R, 97.8% of workers' annual occupational exposures fell within the range of 5 mSv (15).
The results of our study are significantly lower than the suggested international yearly limit for one year (20 mSv) as recommended by ICRP (11) and for a period of 5 consecutive years which were also indicated by Jabeen A et al. (12).
When comparing the results of this study to previous studies, it is clear that there are variations in the radiation doses received by workers in different countries and at different times. For instance, the average occupational exposure data from Jabeen et al. (2003-2007) for medical physics, radiotherapy, and nuclear medicine in Pakistan ranged from 1.05 to 1.80 mSv (12), which is somewhat higher than the ranges observed in our study at CENAR Quetta (0.90 to 1.20 mSv) from 2019 to 2023. This difference could be due to improved radiation protection measures and stricter enforcement of safety protocols over the years. Furthermore, Weizhang et al.reported annual doses in China from 1.2 to 2.2 mSv for similar categories, which are higher than our findings (13). Differences in the types of equipment used, operational procedures, and adherence to safety standards might account for these variations.
Conclusion
This study's primary goal was to assess radiation doses received by radiation personnel in accordance with allowable limits (10, 11). Based on the annual and last five years' dose data of all CENAR Quetta radiation workers, it can be concluded that all radiation workers' radiation doses fell within the acceptable range set by national (10) and international (11) organizations. This confirms the sufficiency of the facilities for radiation protection and demonstrates the rationality of radiation protection techniques (16). The results demonstrate the effectiveness of radiation protection measures and the adherence to safety recommendations in the departments under study, making them clinically meaningful and important. For the purpose of protecting the health of healthcare professionals who are frequently exposed to ionizing radiation at work, this knowledge is essential. The study's findings might also help with ongoing initiatives to optimize radiation exposure in medical settings and guide future modifications to radiation safety procedures. This research contributes to our comprehension of radiation exposure at work in a particular healthcare environment by providing information on radiation levels, trends, and the efficiency of radiation shielding techniques. The data offered is helpful to the larger area of radiation safety in medical practice in addition to being pertinent to the specific context of CENAR.
Limitations and Future Research
Future research should aim to include a larger sample size to improve the representativeness of the findings. Further studies could also explore the long-term health outcomes of radiation exposure among these workers to provide a more comprehensive understanding of the risks involved.
Acknowledgments
The author is cordially thankful to Dr. Hudair Samad for helping me throughout this research.
Ethical statement
The Ethical Review Committee has reviewed and approved the ethical statement associated with the manuscript titled “Occupational Radiation Monitoring Practices in the Southwest Region of Pakistan.” This study complies with ethical guidelines, including obtaining informed consent, ensuring confidentiality, and managing risks, maintaining data integrity, and disclosing conflicts of interest. This approval, letter number Dir-3(17)/24, confirms adherence to the highest ethical standards and supports the publication of your paper.
Data availability
Data will be available as per request.
Author contributions
All Authors contributed equally.
Conflict of interest
The Authors declare no conflict of interest.
Funding/support
Nil
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Address: Urmia University of Medical Sciences, Jahad Ave., Urmia, I.R. Iran. Post code: 57147-83734. P.O. Box. 1138
Email: ijrabms gmail.com
gmail.com
rabmsumsu.ac.ir
Tel / Fax: +984431937332/+984432240642
